Schizotypal Personality Disorder Symptoms Treatment and How It Differs from Schizophrenia
· 15 min read

Introduction
Do you ever feel like your mind works differently than everyone else’s? Maybe you hold strong beliefs that others find odd, or you feel intensely uncomfortable in social settings. For some people, these experiences go beyond being a little quirky. They could be signs of a condition called schizotypal personality disorder (STPD).
STPD is a complex mental health condition that sits on the schizophrenia spectrum. According to the StatPearls clinical resource, it involves a long-standing pattern of social and interpersonal deficits, along with eccentric behavior and odd beliefs. But here is the thing: STPD is not the same as schizophrenia, even though people often confuse the two. The Mayo Clinic notes that those with STPD may have strange thinking or speech, flat emotions, and few close friends, but they do not experience full psychosis like in schizophrenia.
Millions of people around the world live with STPD. Yet stigma and a lack of accurate information keep many from getting the right diagnosis and care.

In fact, the condition is often misunderstood or mislabeled, leading to years of confusion.
In this article, we break down what STPD really is, how it differs from schizophrenia, and which evidence-based treatments can help. To learn more about the key differences between these two conditions, check out our guide on the 5 symptoms of schizophrenia and how they differ from personality disorders.
With so much conflicting mental health news online, it is easy to feel overloaded. Stay informed without the noise. Filter the Noise delivers clear, reliable updates straight to you.
What Is Schizotypal Personality Disorder? Defining Features and Prevalence
Let’s paint a clearer picture. You might know someone who always dresses a bit oddly or talks about ideas that seem strange to most people. Maybe they feel very anxious around others, suspect that people are out to get them for no clear reason, and prefer to spend time alone. This pattern, when it lasts for years, could be schizotypal personality disorder.
Schizotypal personality disorder is a condition where a person has a long-term pattern of social and interpersonal struggles, along with eccentric behavior and odd thinking, according to the StatPearls clinical resource.
The current edition of the diagnostic manual, the DSM-5-TR, places STPD in the schizophrenia spectrum and other psychotic disorders section. This placement highlights its strong genetic and biological links to schizophrenia, even though the two conditions are not the same.
So what does STPD actually look like day to day? The Merck Manuals lists some key features: odd beliefs or magical thinking, such as believing in clairvoyance, telepathy, or a sixth sense. People with STPD might also have unusual perceptual experiences, like sensing a presence in the room that is not there. They often have odd speech patterns, flat or inappropriate emotions, and behavior or appearance that seems peculiar to others. A diagnostic classification study from PMC also notes that a lack of close friends or confidants, along with paranoid thoughts, are central parts of the disorder.
You might wonder how common STPD really is. Research suggests that about 3-4% of the general population has this condition. However, many cases never get officially diagnosed. Why? One big reason is that STPD symptoms can overlap with other mental health issues, like social anxiety disorder, depression, or even early signs of psychosis. It is also often confused with a dissociative disorder, though STPD is fundamentally different. For example, while someone with a dissociative disorder might feel disconnected from their own memories or identity, a person with STPD experiences persistent odd beliefs and social anxiety.
Another reason for underdiagnosis is that people with STPD often avoid seeking help. They tend to be loners who do not want to interact with healthcare professionals. The Mayo Clinic confirms that being a loner and lacking close relationships outside of immediate family is a core symptom. This means many individuals suffer in silence for years.
Understanding the defining features of STPD is the first step. It helps you recognize that these behaviors are not just quirks. They are part of a recognized condition that has real roots in brain function and genetics. To explore how STPD differs from other conditions like dissociative identity disorder, you can read our guide on dissociative identity disorder symptoms and diagnosis.
With so much conflicting mental health information online, it is easy to feel overloaded. Stay informed without the noise. Filter the Noise delivers clear, reliable updates straight to you.
Schizotypal Personality Disorder vs. Schizophrenia: Critical Distinctions
You might hear the terms "schizotypal personality disorder" and "schizophrenia" used interchangeably. That is a common mistake. While they share a genetic link and some overlapping features, they are two different conditions. Getting the diagnosis right matters a lot. It changes the treatment path.
The biggest difference comes down to psychosis.
People with schizotypal personality disorder may have odd beliefs and unusual perceptual experiences, but they usually do not lose touch with reality completely. They often retain at least some insight. They know their strange thoughts are not quite normal. Schizophrenia is different. According to Medical News Today, the main difference is that people with schizophrenia often have full psychotic symptoms.
They experience sustained hallucinations, like hearing voices that seem completely real, and they hold firm delusions that cannot be shaken by logic.
Here is another key point. A person with STPD can usually manage daily life, hold a job, and take care of basic needs. The functional decline seen in schizophrenia is much more severe. Brain scans even show differences. A review in PMC found that the medial temporal lobes and lateral ventricles look normal in STPD, while they often show abnormalities in schizophrenia. That difference in brain structure may help explain why STPD does not progress into the full psychosis that schizophrenia does.
So why does this distinction matter for treatment? It changes the whole approach. Schizophrenia almost always requires antipsychotic medication from the start. STPD, on the other hand, responds best to talk therapy. The Mayo Clinic notes that psychotherapy helps people with STPD build trust, learn social skills, and cope with their odd beliefs. Antipsychotics are used much less often and only in small doses if at all. Misdiagnosing STPD as schizophrenia could lead to unnecessary medication with serious side effects.
This distinction also separates STPD from other conditions. For example, borderline personality disorder (BPD) involves emotional instability and fear of abandonment, not odd beliefs. A person with BPD may have intense mood swings and impulsive behavior, while someone with STPD has persistent eccentric thoughts and social isolation. The DSM-5 criteria for BPD and STPD are very different. And as we noted earlier, STPD is also not a dissociative disorder.
If you want to explore how the signs and symptoms of schizophrenia differ from personality disorders, our guide on the 5 symptoms of schizophrenia and how they differ from personality disorders can help you see the full picture.
Understanding these critical differences can save years of confusion and wrong treatment. Getting a proper evaluation by a qualified mental health professional is the best first step.

Mental health news can feel overwhelming. Stay informed without the noise. Filter the Noise delivers clear, reliable updates straight to you.
Symptoms and Diagnostic Criteria in Depth
Now let’s look closer at the diagnostic criteria that define schizotypal personality disorder. The DSM-5-TR lists nine specific signs. A diagnosis requires at least five of them to be present over time. This pattern must start by early adulthood and show up in different situations.
Here are the nine criteria:
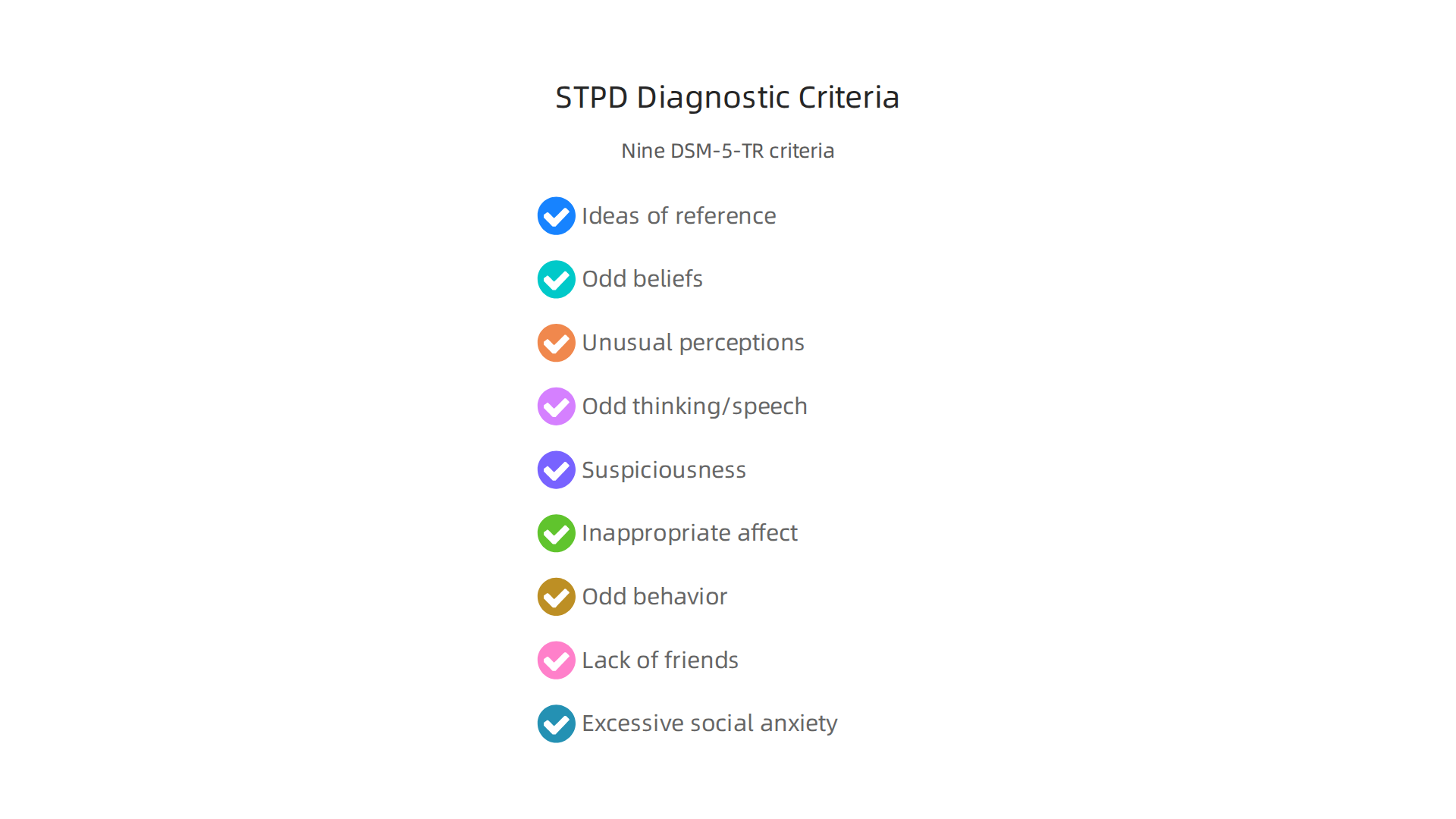
- Ideas of reference. You might think random events have special meaning just for you.
- Odd beliefs or magical thinking. This can include superstitions, belief in telepathy, or feeling you have special powers.
- Unusual perceptual experiences. You may sense a presence that is not there or feel your body is changing.
- Odd thinking and speech. Your words may be vague, metaphorical, or hard to follow.
- Suspiciousness or paranoid thoughts. You may feel others are out to get you, even without evidence.
- Inappropriate or constricted affect. Your emotional reactions do not match the situation, or you seem flat.
- Odd, eccentric, or peculiar behavior and appearance. This can mean wearing unusual clothes or acting in strange ways.
- Lack of close friends. You may have few or no close relationships outside of family.
- Excessive social anxiety. This anxiety does not go away with familiarity and often involves paranoid fears.
These symptoms cluster into three groups. The first is cognitive-perceptual, which includes odd beliefs, unusual perceptions, and suspiciousness. The second is interpersonal, covering social anxiety and lack of close friends. The third is disorganized, involving odd speech and behavior. Each cluster affects daily life in different ways.
Research from PMC shows these symptoms stem from brain differences that are milder than in schizophrenia. The underlying trait of schizotypy connects this condition to a broader spectrum of personality and thought disorders. Studies in Frontiers in Psychiatry also show overlap with schizophrenia across behavioral and neurobiological domains, but the symptoms are less severe.
Getting the diagnosis right means ruling out other conditions. A clinician must check that the symptoms are not better explained by schizophrenia, autism, or another personality disorder. For example, dissociative identity disorder also involves unusual experiences, but the core pattern is different. The same goes for bpd symptoms dsm 5, which focus on emotional instability rather than eccentricity.
Mental health news can feel overwhelming. Stay informed without the noise. Filter the Noise delivers clear, reliable updates straight to you.
Causes and Risk Factors: Genetics, Environment, and Brain Structure
Why do some people develop schizotypal personality disorder while others don’t? That’s a tough question, but researchers have found some important clues. It’s not one single cause. Instead, it’s a mix of genes, life experiences, and brain differences that come together.
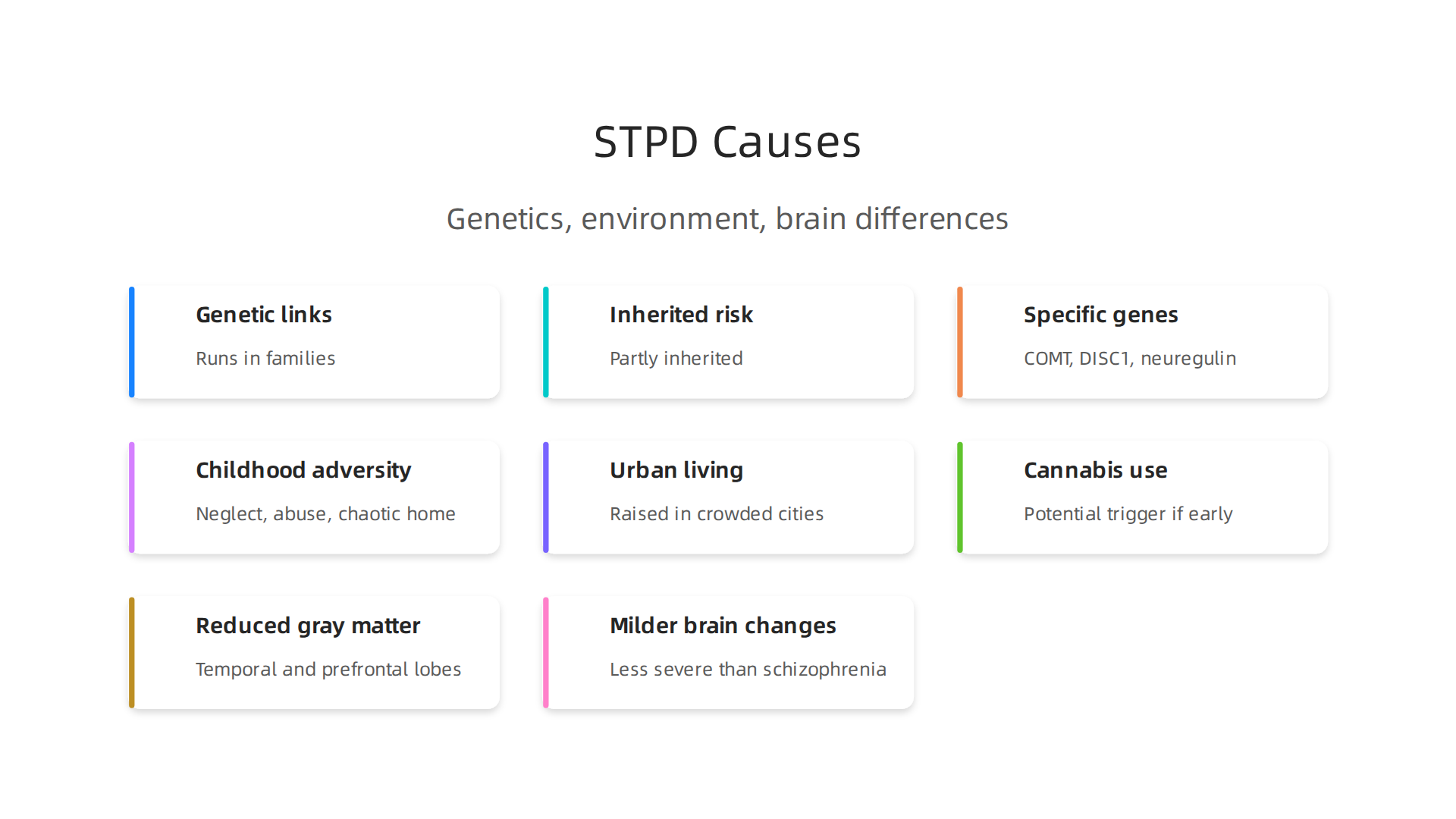
Genetic links
Your DNA plays a big role. Studies on twins and families show that STPD runs in families. The heritability is similar to that of schizophrenia itself. Twin studies, like the one published in JAMA Psychiatry, found that psychotic-like experiences are partly inherited. Specific genes are involved, including variations in the COMT gene, DISC1, and neuregulin. These genes affect how brain cells communicate. If a close relative has schizophrenia, your risk for STPD goes up too. That’s why these two conditions are often called "spectrum" disorders.
Environmental triggers
Genes are only part of the story. The environment shapes how those genes act. Childhood adversity is a major risk factor. Growing up in a chaotic home, experiencing neglect, or facing abuse can increase the chances of developing STPD. Living in a crowded urban area during childhood also raises the risk. Some research points to cannabis use, especially when started young, as a potential trigger. It’s not that any one of these things causes STPD by itself. But when combined with genetic vulnerability, they can push a person toward eccentric thinking and social withdrawal.
Brain structure differences
The brains of people with STPD look different in subtle ways. Neuroimaging scans show reduced gray matter in the temporal lobes, areas that help process sound and language. The prefrontal cortex, which controls planning and social behavior, is also less active. These changes are similar to what you see in schizophrenia, but they are milder. The brain is still trying to compensate, which is why symptoms are less severe.
For a closer look at how schizophrenia symptoms overlap with personality disorders, read our article on the 5 symptoms of schizophrenia and how they differ from personality disorders.
Mental health news can feel overwhelming. Stay informed without the noise. Filter the Noise delivers clear, reliable updates straight to you.
Evidence-Based Treatment Approaches: Psychotherapy and Medication
Living with schizotypal personality disorder can feel isolating, but the good news is that effective treatments exist. A 2026 systematic review published in PubMed confirms that while research is still growing, several evidence-based approaches can make a real difference. Treatment usually combines talk therapy with medication, tailored to each person’s unique symptoms and struggles.
Psychotherapy is the foundation
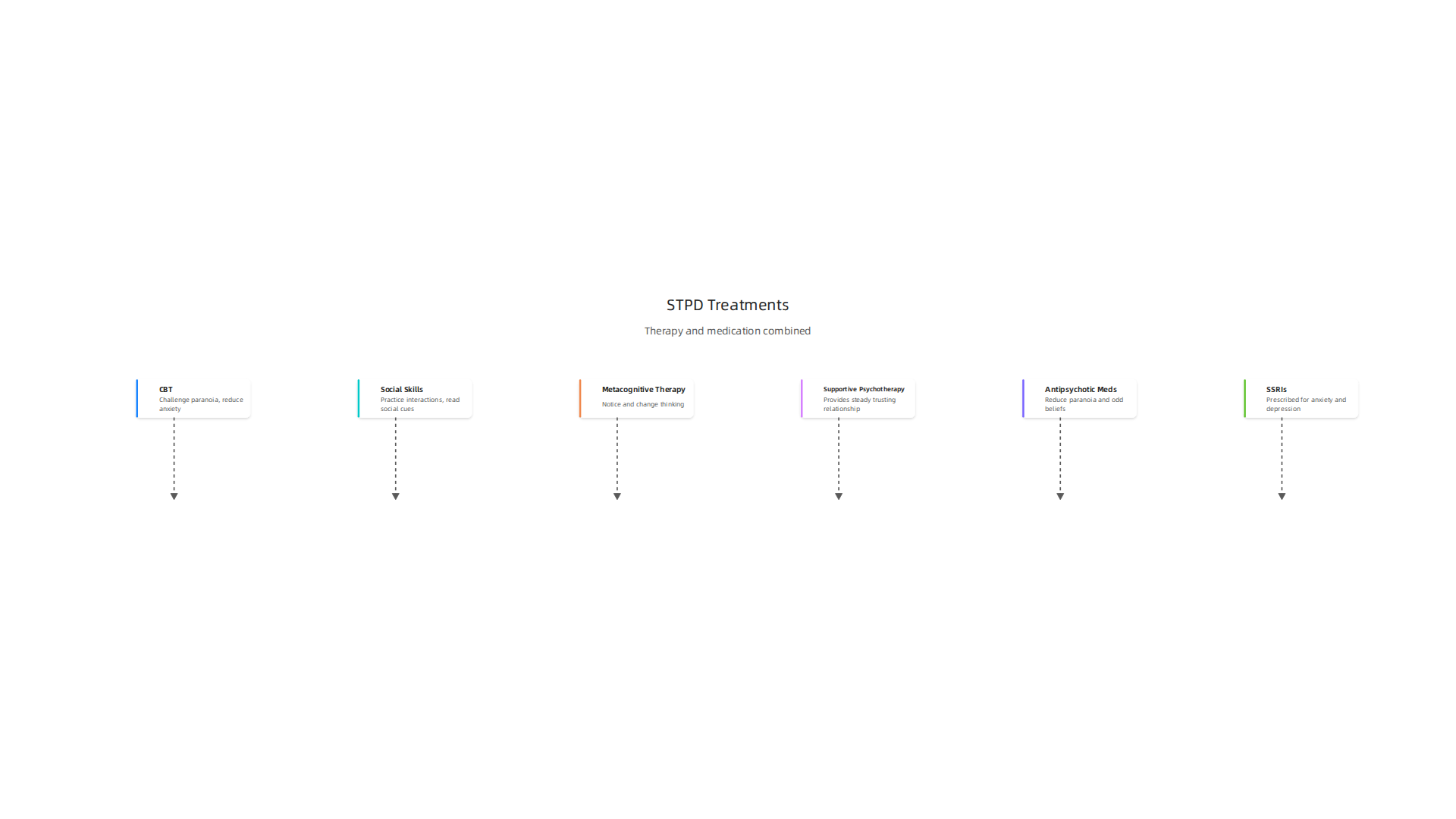
Cognitive-behavioral therapy (CBT) is one of the most studied and helpful therapies for STPD. A therapist trained in CBT can help you challenge paranoid thoughts, reduce social anxiety, and make sense of unusual perceptions. Think of it as retraining your brain’s automatic reactions. The Mayo Clinic notes that CBT is a core part of treatment for many people with STPD. It focuses on practical skills you can use daily.
Social skills training is another powerful tool. It helps you practice everyday interactions in a safe space. You learn how to start conversations, read social cues, and handle awkward moments. Small pilot studies, including those cited in the systematic review, show that this training can reduce social withdrawal and improve relationships.
Metacognitive therapy goes a step deeper. It helps you notice and change how you think about your own thoughts. Instead of getting lost in odd ideas or suspicions, you learn to step back and see them more clearly. The Merck Manual recommends supportive psychotherapy as well, which provides a steady, trusting relationship where you can talk openly.
For more on how CBT helps with conditions that involve social anxiety, read our guide on social anxiety disorder treatment.
Medication plays a supporting role
Medication is not usually the first choice for STPD, but it can be very helpful for specific symptoms.
Antipsychotic medications are used cautiously and at low doses. Drugs like risperidone can reduce paranoid thoughts and odd beliefs. A DrOracle article suggests starting risperidone at just 0.25 mg per day and slowly increasing. These meds are not for everyone. They work best when symptoms are strong enough to get in the way of daily life.
SSRIs (antidepressants) are often prescribed for the anxiety and depression that commonly come with STPD. Feeling down or constantly on edge is exhausting. These medications can lift that weight, making it easier to engage in therapy and build connections.
The key is a team approach. A psychiatrist and therapist work together, adjusting both therapy and meds over time.
What you can do now
If you or someone you care about has STPD, the first step is finding a mental health professional who understands personality disorders. Treatment takes time, but it works.
Mental health headlines can overload judgment. Stay grounded with clear, reliable updates. Filter the Noise delivers the facts you need, straight to you.
Living with Schizotypal Personality Disorder: Coping Strategies and Support Systems
Treatment is essential, but what about the day to day? Living with schizotypal personality disorder means finding ways to manage your thoughts, emotions, and relationships when you are not in a therapist’s office. The good news is that you can build real stability with the right coping strategies and support systems.
Build your support team
A strong support network is one of the best predictors of long-term stability. The 2026 systematic review in PubMed highlights that strong therapeutic alliances and social connections help people stay on track.
Start with your therapist. That trusting relationship is your anchor. Then consider adding a peer support group.

NAMI Connection offers free, peer-led groups where people share experiences without judgment.

Being around others who "get it" reduces isolation and shame.
You might also want to read about building trust in your care team in our article on dissociative identity disorder. The principles of finding safe, supportive professionals apply broadly.
Create a daily coping toolkit
Unusual thoughts and social anxiety can feel overwhelming. Small, consistent habits help you stay grounded.
Mindfulness is a powerful tool. When your mind starts spinning with suspicious thoughts or odd beliefs, a simple breathing exercise can pull you back to the present. Just one minute of focusing on your breath can calm your nervous system.
Stress management is equally important. The Merck Manual notes that reducing overall life stress can ease many STPD symptoms. Try:
- Setting a regular sleep schedule
- Limiting caffeine and alcohol
- Taking short walks when you feel anxious
Structured routines are your friend. When you follow a predictable daily pattern, your brain has fewer chances to wander into odd thoughts. Plan your meals, chores, and relaxation time. This structure reduces decision fatigue and social overwhelm.
Lean on family education (when it feels safe)
Research from the SAMHSA shows that family support can greatly improve outcomes. When family members understand STPD, they are less likely to judge or pressure you. Family psychoeducation sessions teach them how to respond with patience and encouragement.
But here is the hard truth. Stigma often keeps people from telling their families. Many are afraid of being labeled or misunderstood. If your family is not safe to involve, that is okay. You can build your support system with trusted friends, a therapist, and peer groups instead.
Mental health headlines can overload judgment. Stay grounded with clear, reliable updates. Filter the Noise delivers the facts you need, straight to you.
Summary
This article explains schizotypal personality disorder (STPD), a long-term condition on the schizophrenia spectrum marked by odd beliefs, unusual perceptions, social anxiety, and eccentric behavior. It describes the nine DSM-5 criteria used for diagnosis, how clinicians distinguish STPD from schizophrenia and other disorders, and why correct diagnosis matters for treatment choices. The piece reviews genetic, environmental, and brain-structure risk factors linked to STPD and summarizes evidence-based treatments—highlighting psychotherapy (CBT, social-skills and metacognitive approaches) as the foundation, with medication used selectively. Practical guidance covers daily coping tools, building a support team, and family education while noting barriers to diagnosis such as stigma and avoidance. After reading, you’ll understand key symptoms, where to seek help, and the treatment and support strategies that improve functioning and quality of life.