5 Symptoms of Schizophrenia That Distinguish It from Personality Disorders
· 18 min read
If you have ever tried to look up mental health symptoms online, you know how quickly things get confusing. One search might tell you that odd beliefs and social withdrawal point to schizophrenia. Another might say the same signs come from a personality disorder. In 2026, with so much information flying around, it is easy to mix up the two.

Here is the real problem. Misinformation about serious mental health conditions can delay treatment and make things worse. Many people hear about the 5 symptoms of schizophrenia but struggle to separate them from traits linked to avoidant personality disorder or schizoid personality disorder. Even professionals rely on clear guidelines like the ICD-10 mental illness codes to get the diagnosis right. For the average person, that level of detail feels out of reach.
That is where this article comes in. We are going to walk through the five core symptoms of schizophrenia step by step. Then we will look at how personality disorders show up differently and why that distinction matters. Along the way, you will find practical comparisons backed by the latest 2026 research.
To start, it helps to know that schizophrenia has a specific set of criteria. The DSM-5 diagnostic criteria for schizophrenia spells out exactly which symptoms must appear and for how long.
This structure is what separates a clear diagnosis from guesswork.
If you want to go deeper into the official classification, you can read more about understanding the schizophrenia DSM-5 criteria for accurate diagnosis. That page breaks down the timing and symptom requirements in plain language.
Here is the thing. Mental health headlines can overload judgment. When you are trying to understand something as serious as schizophrenia, you need a clean signal. Filter the Noise and focus on facts that actually help you or someone you care about get the right support.
Let us begin with the first symptom.
What Are the 5 Symptoms of Schizophrenia?
Let us get right into the core of it. According to the DSM-5, a diagnosis of schizophrenia requires at least two of the following five symptoms to be present for a significant part of a one-month period. At least one of those symptoms must be delusions, hallucinations, or disorganized speech.
Here are the five symptom domains you need to know.
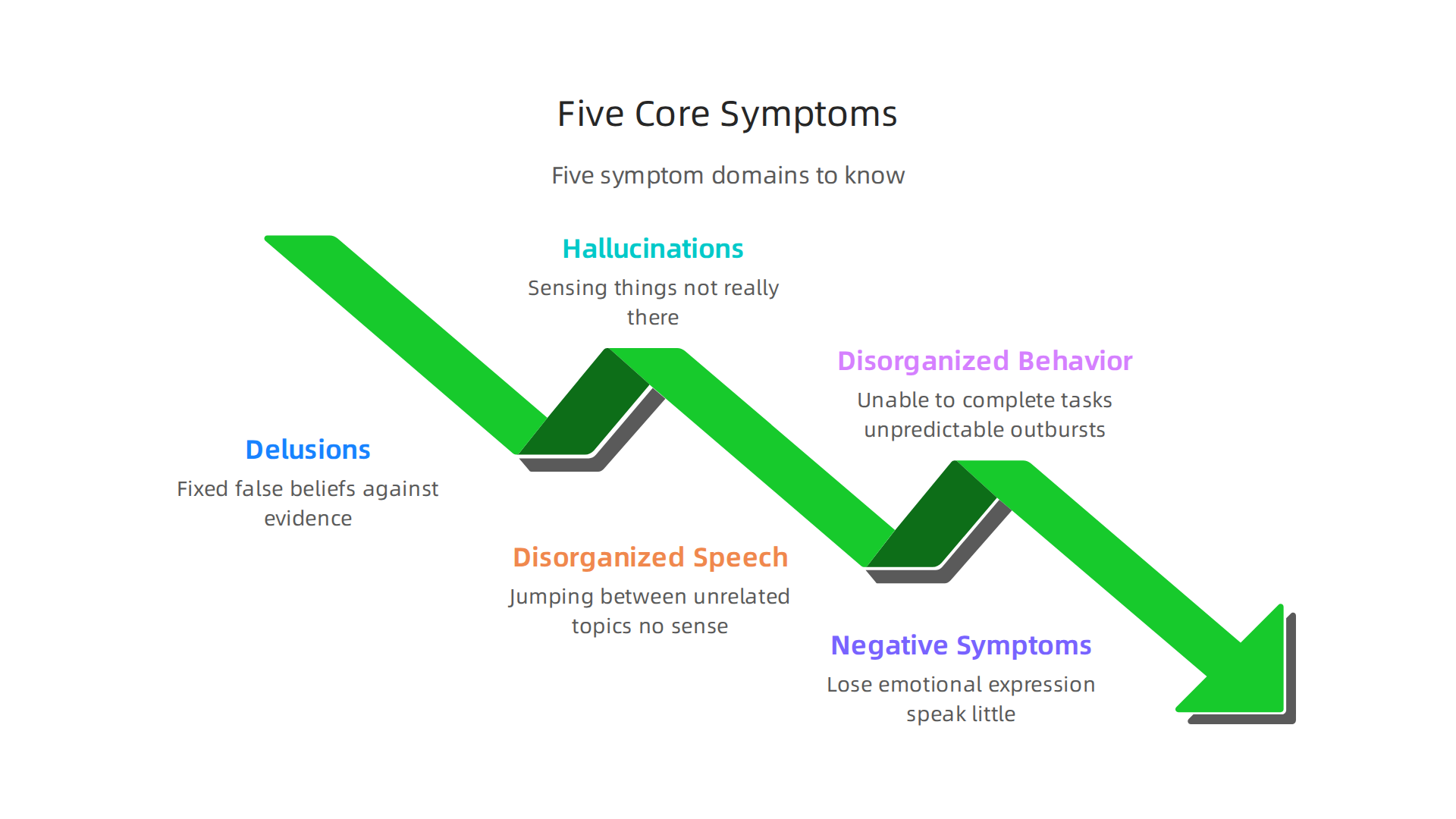
1. Delusions. These are fixed false beliefs that do not change even when there is clear evidence against them. A person might believe they are being watched, followed, or that they have special powers. This is not just being suspicious. Delusions are a break from shared reality.
2. Hallucinations. These involve sensing things that are not really there. Hearing voices is the most common type. The voices may comment on the person’s actions or tell them what to do. Hallucinations can also be visual, like seeing people or objects that do not exist.
3. Disorganized Speech. A person might jump between unrelated topics, string together random words, or speak in a way that makes no sense. This happens because the normal flow of thoughts gets disrupted. It is very different from occasional nervous rambling.
4. Grossly Disorganized or Catatonic Behavior. This can look like many things. A person might be unable to complete everyday tasks like getting dressed or bathing. They may show unpredictable outbursts or move in unusual ways. Catatonia means being completely unresponsive or stuck in a rigid position for a long time.
5. Negative Symptoms. These take things away. A person may lose emotional expression, speak very little, or lose interest in social activities. They might seem flat or withdrawn. These symptoms are often harder to spot than the more dramatic positive ones.
The key here is that these are not personality quirks. They are serious disruptions in how the brain processes reality. And the symptoms must cause major problems in work, relationships, or self-care.
For a closer look at the full diagnostic process, you can check out an schizophrenia overview from NIH that walks through the research.
It also helps to understand how these symptoms differ from traits seen in conditions like avoidant personality disorder or schizoid personality disorder. People with those personality disorders do not lose touch with reality. They have long-standing patterns of behavior that feel normal to them but cause problems. The ICD-10 mental illness classification system draws this line clearly. Schizophrenia involves psychosis. Personality disorders involve deeply ingrained ways of thinking and relating.
If you want to understand the difference at a deeper level, this article on schizotypal personality disorder differences breaks down exactly where the lines blur and how professionals tell them apart.
Now that you know the five symptoms, let us look at how each one shows up in real life and how to tell them apart from similar experiences linked to personality disorders. That is where the real clarity comes in.
How Personality Disorders Are Classified in the DSM-5
You might hear someone say, "He acts a little schizo," and mean it as a casual insult. But that word gets thrown around way too loosely. The truth is, personality disorders are a completely different category from schizophrenia, even though some of them can look similar on the surface.
The DSM-5 groups the ten personality disorders into three clusters based on shared traits.
Think of it like a family tree where each branch has its own flavor.
Cluster A: Odd or Eccentric. This group includes Paranoid, Schizoid, and Schizotypal personality disorders. People with these conditions often seem distant, suspicious, or disconnected from social norms. If you have ever met someone who prefers total isolation and shows almost no emotion, that might point toward schizoid personality disorder. These traits are stable and lifelong, not the acute breaks from reality seen in schizophrenia. For more background on these patterns, you can read about Cluster A Personality Disorders on MentalHealth.com.
Cluster B: Dramatic, Emotional, or Erratic. This cluster includes Antisocial, Borderline, Histrionic, and Narcissistic personality disorders. People here tend to have intense relationships, unstable self-image, and impulsive behaviors. The Cluster B personality disorders overview from Cleveland Clinic explains the four types and their common traits clearly.
Cluster C: Anxious or Fearful. This last group includes Avoidant, Dependent, and Obsessive-Compulsive personality disorders. The core struggle here is chronic worry and difficulty trusting others. Unlike the 5 symptoms of schizophrenia, these patterns do not involve hallucinations or delusions. The ICD-10 mental illness classification system draws the same line: psychosis is the dividing factor.
Here is the key difference that matters most. Personality disorders are stable over time. They develop gradually, often starting in adolescence or early adulthood, and become the person’s way of being. Schizophrenia, on the other hand, involves episodes where reality itself fractures. A person with a personality disorder does not hear voices or believe the government is controlling their thoughts.
If you are trying to figure out whether a loved one has a personality disorder or something more serious, it helps to look at timing. Are the behaviors a lifelong pattern? Or did they start suddenly in young adulthood? That is one of the first clues professionals use.
For a closer look at the full diagnostic classification, you can check out the Overview of Personality Disorders from the Merck Manual. And if you want to see how all this ties back to the 5 symptoms of schizophrenia and where the confusion happens, the article on the 5 symptoms of schizophrenia and how they differ from personality disorders connects the dots directly.
Mental health headlines can sometimes blur the lines between these conditions, which makes it harder to find real answers. If you ever feel like the noise is too much, it helps to Filter the Noise and stick with sources that break things down step by step.
The 5 Symptoms of Schizophrenia vs. Personality Disorder Traits: A Direct Comparison
Now that you understand the clusters, let’s put the 5 symptoms of schizophrenia side by side with the personality disorder traits that sometimes get confused with them. Seeing them together makes the difference much clearer.
The table below shows each core symptom of schizophrenia, a personality disorder trait that can look similar on the surface, and the one major thing that separates them.
| Schizophrenia Symptom | How It Appears in Schizophrenia | Similar Personality Disorder Trait | Key Difference |
|---|---|---|---|
| Delusions | Fixed false beliefs that resist all logic (e.g., "The CIA is tracking me through my fillings"). | Paranoid personality disorder: long-standing distrust and suspicion of others, but beliefs are not firmly fixed. The person can sometimes accept that they might be wrong. | In schizophrenia, insight is lost. The person cannot step back from the delusion. In paranoid PD, the person usually knows their suspicion is excessive even if they cannot shake it. |
| Hallucinations | Hearing voices, seeing things, or feeling sensations that have no external trigger. | Schizotypal personality disorder: odd perceptual experiences like sensing a "presence" or feeling that things are "off," but not full-blown voices. | Hallucinations in schizophrenia are vivid and external. The person believes they are real. In schizotypal PD, the person often describes the experience as unusual and may question it. |
| Disorganized Speech | Jumping from topic to topic with no logical connection, making it hard to follow. | Histrionic personality disorder: dramatic, emotional speech that seeks attention but stays coherent. | In schizophrenia, disorganized speech reflects a breakdown in thought processes. The person cannot control it. In histrionic PD, the speech is intentional and goal-driven. |
| Disorganized or Catatonic Behavior | Childlike silliness, unpredictable agitation, or stiff, unresponsive postures. | Borderline personality disorder: impulsive, self-destructive actions in response to emotional distress, but not truly catatonic. | The disorganized behavior in schizophrenia occurs without a clear emotional trigger. In BPD, it is usually tied to a relationship stressor or intense emotion. |
| Negative Symptoms | Flat facial expression, monotone voice, lack of motivation, social withdrawal. | Schizoid personality disorder: a lifelong pattern of preferring solitude and showing little emotion. | In schizophrenia, these symptoms represent a loss of previous function. The person used to be engaged. In schizoid PD, the person has always been this way and does not feel distressed by it. |
This comparison shows why diagnoses are tricky. Someone with avoidant personality disorder may avoid social situations because they fear rejection. Someone with schizophrenia may withdraw because they are responding to internal voices. The surface behavior looks the same, but the inner experience is worlds apart.
The DSM-5 criteria for schizophrenia require that these symptoms cause a significant drop in functioning and last for at least six months. That timeline is a huge clue. If a pattern has been present for years without worsening, it is more likely a personality disorder. If it appears suddenly in a person’s twenties and comes with a loss of reality testing, schizophrenia is a stronger possibility.
For a deeper look at the diagnostic framework, you can read the full schizophrenia DSM-5 criteria from MentalHealth.com. And if you want to understand how schizotypal personality disorder sits in the gray zone, the guide on schizotypal personality disorder symptoms breaks down that specific overlap.
Here is the bottom line. The 5 symptoms of schizophrenia involve a break from shared reality. Personality disorder traits are rigid but the person still knows what is real and what is not. That single difference changes everything about treatment and outlook.
Why Misdiagnosis Happens and How to Avoid It
You might think that once you spot the 5 symptoms of schizophrenia, a diagnosis is simple. But the table above shows how easily these symptoms can look like personality disorder traits. And that is where real trouble starts.
Misdiagnosis is not rare. It is actually very common.

A study from Johns Hopkins Medicine found that about half of people who came to their clinic with a schizophrenia diagnosis did not actually have it. They had something else, often a mood disorder or a personality disorder. Another study reported that more than a third of people with severe psychiatric disorders were initially misdiagnosed. That is a staggering number of wrong labels.
So why does this keep happening?
Symptom overlap is only part of the story. Yes, a person with avoidant personality disorder may withdraw from others, just like someone with schizophrenia who is responding to voices. And a person with schizoid personality disorder shows little emotion and prefers solitude, which can look like negative symptoms. But the bigger problem is that clinicians often do not have enough information.
Lack of a comprehensive history is a major factor. A doctor might see a patient for 30 minutes and make a judgment based only on what the patient says in that moment. If the patient is distressed and reports hearing a voice, the clinician may jump to schizophrenia. But they miss the full picture. They do not know that the patient has had odd beliefs and social discomfort since childhood, which points toward schizotypal personality disorder instead.
Clinician bias also plays a role. Research from Rutgers University showed that African Americans with severe depression are more likely to be misdiagnosed with schizophrenia than white patients with the same symptoms. Racial bias, along with a lack of cultural understanding, can push a diagnosis in the wrong direction.
The specific risk goes both ways. Schizophrenia can be misdiagnosed as borderline personality disorder when the person shows emotional outbursts. And borderline PD can be misdiagnosed as schizophrenia when the person has brief stress-related paranoia. The same confusion happens with schizotypal PD.
How to Avoid These Mistakes
The best way to get the right diagnosis is to slow down and gather more data.
Use structured interviews. Tools like the Structured Clinical Interview for DSM-5 (SCID) ask standard questions that reduce personal bias. They force the clinician to check every symptom systematically.
Get collateral information. Talking to family members or close friends can reveal whether the person was always socially distant (schizoid PD) or suddenly changed in their twenties (schizophrenia). That piece of history is gold.
Watch the timeline. Symptoms that appear suddenly in young adulthood and come with a loss of reality testing point toward schizophrenia. A lifelong pattern of odd thinking without a clear break points toward a personality disorder.
If you or someone you care about is navigating this confusing space, learning the official criteria can help you ask better questions. The guide on understanding the schizophrenia DSM-5 criteria for accurate diagnosis walks through what clinicians are supposed to check.
Knowing these rules gives you power in your own care.
Getting the right diagnosis matters because treatment is completely different for schizophrenia versus a personality disorder. Wrong label, wrong path. But with the right information and a careful process, misdiagnosis can be avoided.
Latest Research and Diagnostic Tools in 2026
The previous section showed how easily the 5 symptoms of schizophrenia can be confused with personality disorder traits. That confusion is real, but it does not have to be permanent. In 2026, researchers and clinicians have more tools than ever to tell them apart. These new tools are changing the game for accurate diagnosis.

Neuroimaging is getting smarter. Functional MRI (fMRI) scans can now show brain activity patterns that are common in schizophrenia but not in personality disorders. When combined with artificial intelligence, these scans can catch subtle differences that the human eye would miss. A recent review on AI-enhanced fMRI analysis for schizophrenia shows how machine learning can identify brain connectivity patterns linked to the disorder. This means a brain scan might one day help confirm whether someone has schizophrenia or a condition like schizoid personality disorder.
Digital phenotyping is another breakthrough. This sounds complicated, but it is simple. Your phone can track things like how fast you type, how often you move, and your sleep patterns. For someone with schizophrenia, these digital markers often change during a psychotic episode. For someone with avoidant personality disorder, the pattern is different and more stable. Researchers are testing these tools to catch early signs before a full episode happens.
Genetic testing is also advancing. While there is no single gene for schizophrenia, certain risk patterns are becoming clearer. A new study from Northwestern University found a biomarker for cognitive symptoms of schizophrenia that could lead to better treatment and earlier diagnosis. This kind of research may soon help doctors separate schizophrenia from personality disorders at a biological level.
The DSM-5-TR has made important updates. The latest version of the diagnostic manual includes the Alternative Model for Personality Disorders (AMPD). This model asks clinicians to rate how much a person struggles with self-functioning and interpersonal relationships. It also rates the severity of specific personality traits. This system is much more precise than the old method of just checking boxes. For example, someone with schizotypal personality disorder would show odd thinking and eccentric behavior, but not the hallucinations or delusions that define schizophrenia. The AMPD helps draw that line clearly.
AI-assisted differential diagnosis is becoming a reality. Machine learning models can now take in a patient’s history, symptom checklist, and even speech patterns to suggest the most likely diagnosis. A 2026 review in Frontiers in Psychiatry describes how artificial intelligence approaches for schizophrenia prediction are improving accuracy. These tools are not meant to replace doctors, but to help them avoid the bias and shortcuts that lead to misdiagnosis.
If you want to see how the classic symptoms compare across disorders, the guide on the 5 symptoms of schizophrenia and how they differ from personality disorders breaks it all down. Knowing the difference can save years of the wrong treatment.
Practical Steps for Seeking Accurate Diagnosis and Care
So, how do you make sure you get the right diagnosis? It starts with a thorough psychiatric evaluation.

Here is what to expect and how to advocate for yourself.
What to expect from a psychiatric evaluation. A good evaluation for schizophrenia or a personality disorder usually takes several appointments. Your provider will ask about your symptoms, your medical history, and your family background. They will want to know when symptoms started and how they affect your daily life. They will also rule out other causes like substance use or medical conditions. The Mayo Clinic guide on personality disorders explains that personality disorders involve long-term patterns of thinking and behavior, while schizophrenia includes psychotic symptoms like hallucinations. That distinction is key. Doctors often use the DSM-5 and ICD-10 codes to record a diagnosis. For example, the StatPearls overview of personality disorders details the specific DSM-5-TR criteria for each condition. Knowing these can help you ask informed questions.
Questions to ask your provider regarding differential diagnosis. Do not be shy. Ask directly: "What is your differential diagnosis?" This means asking what other conditions could explain your symptoms. For example, the 5 symptoms of schizophrenia include delusions and disorganized speech, but avoidant personality disorder involves fear of rejection, not psychosis. You can also ask: "Could this be schizoid personality disorder or schizotypal personality disorder instead?" A good clinician will walk you through their reasoning. For a deeper look, you can read our guide on understanding the schizophrenia DSM-5 criteria for accurate diagnosis.
The importance of second opinions and specialized clinics. Misdiagnosis is common, especially between schizophrenia and cluster A personality disorders. If something feels off, get a second opinion. Specialized clinics that focus on psychotic disorders or personality disorders have more experience with these tricky cases. They use tools like structured interviews and may take more time to observe your symptoms over weeks or months. Some hospitals offer differential diagnosis programs where a team of experts reviews your case. The right diagnosis saves time, money, and emotional pain.
Remember, you are your own best advocate. With so much information online, it helps to Filter the Noise and stick with reliable sources. The right diagnosis leads to the right treatment. And that changes everything.
Summary
This article explains the five core symptom domains of schizophrenia—delusions, hallucinations, disorganized speech, grossly disorganized or catatonic behavior, and negative symptoms—and shows how they differ from similar traits in personality disorders. It walks through DSM-5 criteria, the importance of timing and loss of reality testing, and why personality disorders (like schizoid, schizotypal, or avoidant) are distinct despite surface overlap. The piece highlights why misdiagnosis happens, common clinician pitfalls, and practical steps patients and families can take to get a correct diagnosis. It also surveys 2026 advances—AI-enhanced fMRI, digital phenotyping, and genetic biomarkers—that are improving differential diagnosis. Throughout, the article gives clear comparisons, examples, and actionable advice on what to ask clinicians and when to seek second opinions, so readers can pursue the right treatment pathway faster.