Dissociative Identity Disorder Symptoms Causes and Evidence Based Treatments
· 17 min read

Understanding Dissociative Identity Disorder: More Than a Diagnosis
You have probably seen dissociative identity disorder in movies or true crime shows. But what you saw was likely wrong. The real condition is nothing like the Hollywood version that grabs headlines.
DID is often misunderstood. That misunderstanding leads to stigma. And stigma leads to delayed diagnosis. Many people suffer for years without knowing what is really going on.
Here is a number that might surprise you. DID affects about 1 to 3 percent of the general population. That makes it as common as some conditions you hear about much more often. Yet it remains one of the most underdiagnosed disorders in mental health. The National Institutes of Health notes that this condition is often misdiagnosed and usually requires multiple assessments before a correct diagnosis is made, as shown in the StatPearls overview on dissociative identity disorder.
The confusion makes sense. DID involves two or more distinct personality states along with gaps in memory. But the symptoms can look like other conditions.

That is why understanding the medical terminology matters. Without accurate information, people miss out on the help they need.
This article gives you a complete evidence-based look at dissociative identity disorder. We will cover the symptoms, how doctors diagnose it, what causes it, and which treatments actually work. We will also talk about newer support frameworks that are changing how people live with DID.
If you are here because you or someone you care about might have DID, you are in the right place. Mental health news can overwhelm anyone. When the headlines get loud, you can go to Deangrey.org to filter the noise and find clear information.
Let us start with the basics. Because understanding DID begins with knowing what it really is and what it is not.
What Is Dissociative Identity Disorder?
So what exactly is dissociative identity disorder according to the official medical guidance? The DSM-5, which is the main manual doctors use to diagnose mental health conditions, defines DID as a disruption of identity. That disruption involves two or more distinct personality states. These states are often called alters. Each one can have its own way of thinking, feeling, and behaving.
The condition also comes with memory gaps.
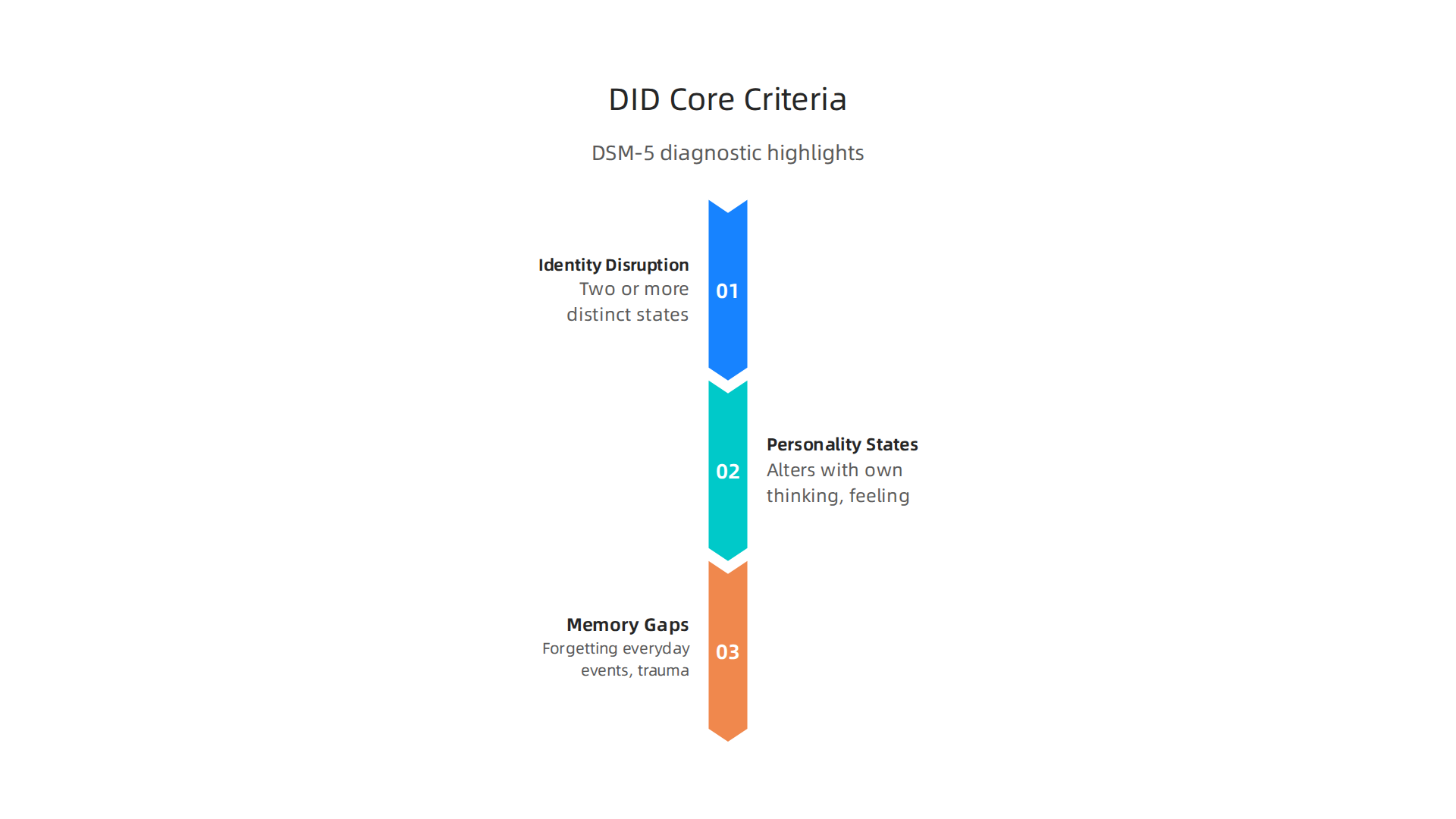
People with DID may forget everyday events, personal information, or even past trauma. These are not just normal forgetfulness. They are real breaks in recall that affect daily life.
You can find the full diagnostic criteria for dissociative identity disorder on the Psychiatry.org page on dissociative disorders.
The symptoms listed there include the existence of two or more distinct identities, along with recurring gaps in memory that are too big to be explained by ordinary forgetting.
The name of this condition has changed over time. You might have heard it called multiple personality disorder. That older name was used for decades. But in 1994 the medical community changed it to dissociative identity disorder. The switch was not just about sounding more professional. It reflected a deeper understanding of what is really happening. The new name highlights dissociation, which is the core problem. People do not really have separate personalities living in one body. Instead, their sense of self has become fragmented, usually because of severe trauma. The PMC article on multiple personality disorder and dissociative identity disorder explains this shift in medical terminology.
Understanding these basics matters. It helps you spot the difference between DID and other conditions like schizoaffective disorder, which can look similar from the outside but has a very different cause and treatment path.
If you want to go deeper into the symptoms and how doctors make the diagnosis, check out our guide to dissociative identity disorder on Mental Health News Today. It breaks down the rest of the DSM-5 criteria in plain language.
Now that you know what DID is, let us look at the signs that someone might be living with this condition. That is where things start to make more sense.
Symptoms and Clinical Presentation
So what does dissociative identity disorder actually look like in daily life? The symptoms go deeper than most people realize. They are not just about switching between identities like in movies. Real DID is often quiet, confusing, and exhausting.
Core Symptoms to Know
The main symptom is having two or more distinct personality states, often called alters. Each alter can have its own name, age, gender, memory, and even voice. Some alters may be children. Others may be protectors or persecutors. The Types of Alters in DID guide explains the different roles these parts can take.
Along with alters, people with DID experience gaps in memory. They might forget conversations, hours of time, or important personal events. This is not normal forgetfulness. It is amnesia linked to the switch between states. Many people also feel confused about who they really are. This is called identity confusion.
Common Conditions That Overlap
DID rarely appears alone. Most people with this condition also struggle with other mental health problems. Post-traumatic stress disorder (PTSD) is the most common one. In fact, the Dissociative Subtype of PTSD is a specific form where people feel detached from their own body or the world around them. Depression and anxiety disorders are also very common.
This overlap can make diagnosis tricky. A doctor must tell the difference between DID and other conditions like schizoaffective disorder or borderline personality disorder. That is one reason the medical terminology around DID has become more precise over time.
How It Affects Daily Life
The impact of DID can range from mild to severe. Some people manage to hold jobs and maintain relationships. Others face serious struggles.

Work performance may suffer due to lost time or confusion. Relationships become hard because partners do not always understand the changes in personality or mood.
The Dissociative Identity Disorder DID Knowledge Center describes how a unified sense of self gets broken. This fragmentation can make it hard to feel like one whole person from day to day.
If you or someone you know is dealing with these symptoms, understanding them is the first step. Learning how to cope with the emotional ups and downs of dissociation can make a real difference. Our guide to therapy for emotional regulation covers practical strategies that help with managing intense feelings and staying grounded.
Now that you know the signs, the next part is understanding how doctors actually test for and confirm DID. That process is more careful than you might expect.
Diagnostic Challenges and Common Misdiagnoses
Getting the right diagnosis for dissociative identity disorder is harder than it should be. Many people wait years before a doctor correctly identifies their condition. In the meantime, they often receive the wrong label and the wrong treatment.
Why DID Gets Missed
The biggest problem is how much DID looks like other conditions. A person might show rapid mood swings, memory gaps, or hearing voices. Each of these symptoms points to something else. Doctors often first suspect borderline personality disorder because of emotional ups and downs. Bipolar disorder gets suggested when energy levels shift. And paranoid or unusual thoughts can look like schizophrenia. Good research on DID and common misdiagnoses confirms how often these errors happen.
The medical terminology around dissociative disorders has changed over time too. Older names like multiple personality disorder made people think DID was rare or fake. That skepticism still exists today. Many clinicians receive little training on dissociation during medical school. So when they see a patient with confusing symptoms, they pick a more familiar diagnosis instead.
The Cost of Being Misdiagnosed
Getting the wrong diagnosis means getting the wrong help. Someone told they have bipolar disorder may take mood stabilizers that do nothing for DID. A person labeled with schizophrenia might receive antipsychotics that only treat some symptoms. Meanwhile, the real issue trauma and dissociation goes unaddressed. This delay can make things worse over time.
A careful assessment makes all the difference. Doctors who use the Structured Clinical Interview for Dissociative Disorders (SCID-D) catch DID much more accurately. This interview asks specific questions about memory, identity confusion, and detachment. It rules out similar looking conditions like schizoaffective disorder.
If you want to understand how professionals tell these conditions apart, the schizophrenia DSM-5 criteria explain the key differences between dissociation and psychosis. Knowing these distinctions helps you ask better questions during your own evaluation.
The path to a correct diagnosis takes patience. But with the right tools and an open minded clinician, it is absolutely possible to get clarity.
Root Causes and Risk Factors
You might wonder why one person develops dissociative identity disorder while another does not. The answer almost always points back to childhood.

DID does not appear out of nowhere. It is a direct response to overwhelming pain during the early years of life.
Severe Childhood Trauma is the Main Cause
The clearest link is repeated and severe trauma during childhood. Physical abuse, sexual abuse, and emotional abuse create an environment where the developing mind cannot cope. To survive, the child’s mind splits off parts of experience into separate identities. This is not something that happens after one bad event. It happens after ongoing, long-term trauma.
According to the Mayo Clinic, individuals who experience long-term physical, sexual, or emotional abuse during childhood are at the highest risk for dissociative disorders. The estimated number is striking: around 90% of people with DID report a history of severe childhood trauma. The trauma must be both intense and repeated for dissociation to become a permanent way of coping.
Attachment Disruptions and Cumulative Stress
Trauma alone does not tell the whole story. A child needs a safe caregiver to help them make sense of scary experiences. When that bond is broken by neglect, inconsistency, or the caregiver being the source of abuse, the child cannot develop healthy attachment. Research from the National Institutes of Health shows that disruptions in early attachment and cumulative stress are strongly linked to dissociative symptoms later in life.
Children who lack emotional and social support are more likely to dissociate. Without someone to comfort them, the mind learns to handle pain on its own by separating from it. That survival strategy works in the moment but carries long-term costs.
What Happens in the Brain
Repeated trauma does not just change a child’s emotions. It changes the brain’s physical structure. Studies have found reduced hippocampal volume in people with DID. The hippocampus is the part of the brain that helps form and store memories. When it shrinks, memory gaps and identity confusion become more severe.
Understanding these root causes can help you make sense of your own experiences or those of someone you love. If you want a deeper walkthrough of the full picture, check out this guide to understanding dissociative identity disorder symptoms and treatment options. It covers how these early risks connect to real-world care.
Evidence-Based Treatment Approaches
If you or someone you love is living with dissociative identity disorder, you need to know this: real, effective help exists. Treatment for DID follows a structured, research-backed path that helps people heal without rushing into painful memories before they are ready.
The Phased Treatment Model
Experts agree that DID treatment works best in three clear stages. This is called phasic treatment, and it is the gold standard for care.
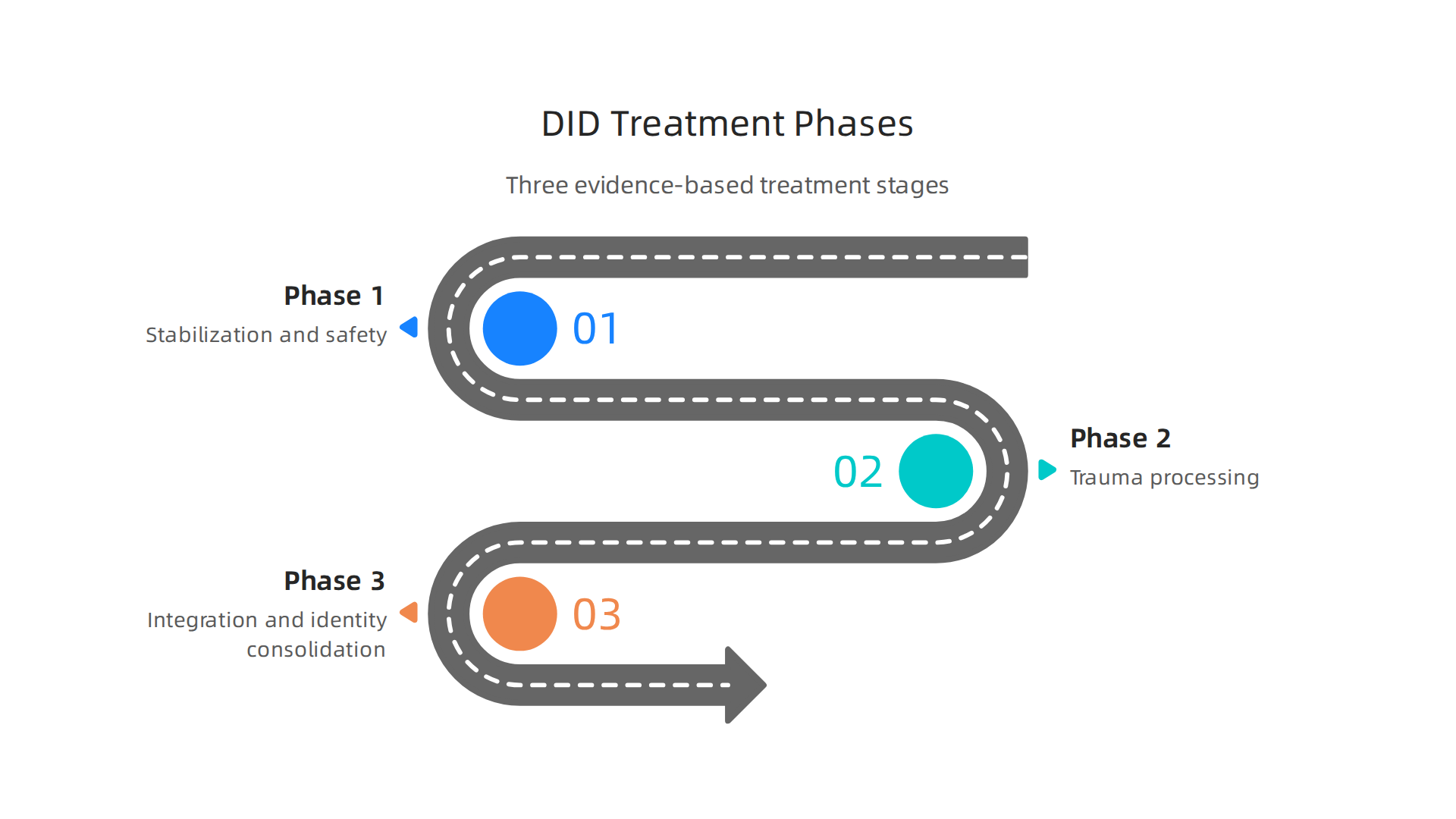
According to research from DID-Research.org, current evidence strongly supports this phased approach as the most effective way to improve symptoms over time.
Phase 1: Stabilization and Safety
This first stage is all about building stability. The goal is to help you feel safe in your body and your life. You learn coping skills to manage flashbacks, emotional overwhelm, and self-harm urges. Grounding techniques and distress tolerance become your daily tools. This phase can take months or even years, and that is completely normal. Rushing this part can make things worse.
Therapies that work well here include cognitive behavioral therapy (CBT) and dialectical behavior therapy (DBT). Both help you build emotional regulation skills without diving into trauma details yet.
Phase 2: Trauma Processing
Once you are stable, the work of processing traumatic memories begins. This does not mean reliving every painful moment. Instead, you work with a trained therapist to gently integrate those memories into your full life story. Approaches like EMDR and sensorimotor psychotherapy are often used here. These methods focus on how trauma lives in the body as well as the mind.
Recent findings from a 2025 study published in Frontiers in Psychiatry confirm that evidence-based developments continue to improve how clinicians approach this delicate stage.
Phase 3: Integration and Identity Consolidation
The final phase is about bringing all parts of yourself together. The goal is not to erase the different identities but to help them cooperate and eventually merge into a unified sense of self. This takes time, patience, and a strong therapeutic relationship.
What about Medication?
Here is something important to understand. No medication treats dissociative identity disorder directly. However, many people with DID also struggle with depression, anxiety, or sleep problems. Medications can help manage those co-existing symptoms. Your doctor might prescribe antidepressants or mood stabilizers to support your overall treatment plan, but the real healing happens through therapy.
If you want to learn more about how standard treatment approaches fit into the bigger picture of mental health care, check out this guide on understanding dissociative identity disorder symptoms diagnosis and treatment. It pulls together everything from diagnosis to long-term recovery in one place.
Innovative Frameworks for Mental Health Support
Beyond these well-established treatment stages, new frameworks are emerging that can make the healing process even more effective. One such approach is the Value Reinforcement System (VRS). This patented framework uses recognition and positive feedback to shape healthy behaviors over time. Instead of focusing on problems, it builds up what works.
How VRS Complements DID Treatment
You might wonder how a reinforcement system fits with trauma care. The answer is simple. The stabilization phase of dissociative identity disorder treatment is all about building safety and trust. VRS directly supports that goal. By rewarding small wins and consistent coping behaviors, it helps the brain form new, positive patterns. This can offset the anxiety and depression that often come with DID.
Research shows that DID symptoms improve when treated using a structured trauma-focused approach. Adding a behavioral reinforcement layer like VRS can make that progress steadier and more lasting.
Building Safety Through Positive Reinforcement
Think of it this way. When you learn to ground yourself during a flashback, that is a huge achievement. VRS makes sure that achievement gets recognized. Over time, your brain starts to expect that recognition. It becomes a motivator to keep using healthy skills.
Learning to regulate your emotions is a core part of this process. If you want practical strategies for building those skills, check out this guide on therapy for emotional regulation. It walks you through methods that work well alongside trauma-informed care.
The VRS framework is protected under a U.S. patent. You can explore the details of the VRS Patent 12,205,176 to understand the science behind how recognition can rewire behavior. It is one example of how modern mental health news is moving beyond traditional talk therapy into tools that shape daily habits.
This kind of innovation does not replace the phased treatment model. It strengthens it. And for anyone living with dissociative identity disorder, having more tools in the toolbox means more hope for lasting recovery.
Living with DID: Practical Strategies and Building Resilience
Living with dissociative identity disorder can feel overwhelming some days. But you don’t have to face it without a plan. Small, consistent strategies can make a big difference in how you manage daily challenges.
Start with grounding techniques. Simple actions like naming five things you see, placing your feet flat on the floor, or holding something cold can pull you back when you feel disconnected. Combine those with a basic self-care routine: regular sleep, meals, and short breaks. Learning about your condition also helps. This is called psychoeducation. Knowing that dissociative identity disorder often develops as a response to severe childhood trauma can reduce shame and confusion. A clear explanation of what causes DID can be a powerful first step in your healing journey.
Support from others matters just as much. A trusted therapist, a close family member, or a support group can help you stay on track. Sticking with your treatment plan even on tough days is key to steady progress. If you want a deeper look at how diagnosis and effective treatment work, this guide on dissociative identity disorder understanding symptoms diagnosis and effective treatment walks you through the process.
Innovative tools can also reinforce the positive habits you build in therapy. The Value Reinforcement System uses recognition to reward healthy behaviors like grounding or reaching out for help. Over time, your brain learns to expect that positive feedback, which makes it easier to keep using good coping skills. The practical results of this approach for offsetting anxiety and depression were highlighted in a feature by Authority Magazine. It shows how shaping and rewarding healthy behaviors can build real resilience over the long haul.
The Future of DID Research and Care
Looking ahead, researchers are making exciting progress in understanding dissociative identity disorder. New studies using brain imaging and genetic testing may soon help doctors diagnose DID more accurately and predict which treatments will work best for each person.

The goal is to move beyond guesswork and offer care that is truly personalized.
Digital tools are also changing the picture. Apps and online platforms can deliver therapy support and behavioral reinforcement directly to your phone. This makes it easier for people who live far from specialists or who cannot afford frequent visits to still get quality care.
Reducing stigma remains a top priority. Many clinicians still lack proper training on dissociative identity disorder, which leads to missed diagnoses. A global conference on DID recently brought experts together to break down these barriers and improve education for providers. You can read more about the global conference on dissociative identity disorder and how it aims to change the conversation.
If you want to stay informed about the latest research and awareness efforts, check out the Mental Health Awareness Month 2026 guide for updates on campaigns and new studies.
Summary
This article offers a clear, evidence-based guide to dissociative identity disorder (DID), explaining what the condition really is, how common it is, and why popular portrayals are misleading. It covers the DSM-5 definition—two or more distinct identity states plus memory gaps—typical symptoms, and the frequent overlap with PTSD, depression, and anxiety that complicates diagnosis. The piece explains why DID is often missed or misdiagnosed, outlines the dominant causes (especially repeated childhood trauma and attachment disruption), and describes the phased treatment model clinicians use: stabilization, trauma processing, and integration. It also clarifies the limited role of medication, introduces newer support tools like the Value Reinforcement System (VRS), and offers practical grounding and resilience strategies for daily life. Finally, the article looks ahead to advances in research, digital care options, and efforts to reduce stigma so people get accurate diagnoses and better care.